German
historian Götz Aly is an expert on euthanasia during the Nazi era. In a SPIEGEL
interview, he discusses why many accepted the murder of the handicapped and
mentally ill, and how his own daughter has shaped his views on how the disabled
should be treated today.
Some 200,000
people who were mentally ill or disabled were killed in Germany during the Nazi era. The cynical name for
the extermination program was "euthanasia," which means
"beautiful death" in ancient Greek. This horrific past has shaped the
way Germany treats the terminally ill and the disabled. Germany's laws on assisted suicide are
restrictive, and the country has stricter rules on pre-implantation genetic
diagnosis, a form of embryo profiling, than most other European countries.
In 2006, the
United Nations General Assembly adopted the Convention on the Rights of Persons
with Disabilities, which Germany ratified in 2009. It calls for a
so-called inclusive education system for all children, which means that
children with disabilities and behavioral disorders should be allowed to attend
mainstream schools. The German city-state of Bremen adopted the inclusion requirement in
2009, and other German states are in the process of implementing it.
Now a debate has unfolded on the
pros and cons of inclusion. Proponents say that being different has to become
normal. But opponents believe that inclusion comes at the expense of
special-needs schools, that teachers are overwhelmed, that better students are
short-changed, and that disabled children feel excluded in mainstream classes.
It is a debate in which some are
berated as idealists and others as ideologues. But, ultimately, the real issue
is how to define the moral standards of coexistence.
Berlin contemporary historian Götz Aly, 65, has a 34-year-old
disabled daughter named Karline. In a SPIEGEL interview, he talks about the
joys and hardships of everyday life with a disabled child. Aly has spent 32
years studying the issue of euthanasia. His book,
"Die Belasteten" ("The Burdened"), was recently published
by the S. Fischer publishing house.
SPIEGEL: Mr. Aly, you
have studied the murders of the disabled and mentally ill in the Nazi era, or
what was then referred to as "euthanasia." Didn't the issue strike a
little too close to home for you?
Aly: I know, of course, that my daughter would have been one of
the candidates for murder at the time. But Karline's illness 34 years ago was
precisely the reason I approached the subject in the first place. Perhaps it
was also a way for me to come to terms with it. That's what brought me to study
the Nazis. It doesn't bother me when issues affect me personally. On the
contrary, it bothers me that many Germans who write about the Nazi period
behave as if they have no personal points of reference. I sometimes amuse
myself by asking older colleagues: "Now what exactly did your father do in
World War II?"
SPIEGEL: Your book about euthanasia is dedicated to Karline, and you
also write a few sentences about her. Nevertheless, your daughter is hardly
mentioned in reviews and interviews. Is there a reluctance there?
Aly: It's an academic book, and it's discussed under academic
criteria. German historians cultivate so-called objectivity. They persuade
themselves that they can switch off the subjective and therefore the
unsettling. But there is one German history professor who regularly asks me how
Karline is doing, and that's Hans Mommsen (a leading expert on Nazi Germany and
the Holocaust). That sets him apart from the others.
SPIEGEL: How
does the reluctance to talk about personal matters affect academic research?
Aly: I
am both on the edge of the academic community and in a somewhat tense
relationship with it -- a relationship from which I derive energy, inspiration
and questions. A large part of this community is unthinkingly self-involved,
producing reams of sterile writing -- often consuming unbelievable amounts of
public funds -- and serving as an instruction manual for how to chase away
readers and ignore historical insights. Much of the research on the Nazi era
makes a science out of distancing oneself from it or conjuring its demons. The
conceit is that people were monsters then -- as if they were completely
different from people today.
SPIEGEL: Where are there commonalities?
Aly: The subtitle of my new book is: "A History of
Society." I don't just look at the 500 murderers and 200,000 euthanasia
victims. Instead, I try to shed light on what was going on around them. For
instance, how did family members and neighbors behave? When you take this
approach, you encounter reactions that are universally human. The chronically
ill and the disabled can become a burden for families. No one is unfamiliar
with this experience.
SPIEGEL: Hence the title of your book: "The Burdened." You
demonstrate that killings on such a massive scale would not have been possible
without the tacit consent of family members.
 |
| T-4 Nazi euthanasia center. |
Aly: I
wouldn't call it consent. The organizers of the euthanasia murders
systematically asked how often a patient was visited, and by whom. If they had
the impression that a family was not very close-knit, the sick person was taken
away far more quickly than someone who received regular visits. After the
murder, the relatives received an official death certificate with a fabricated
cause of death. Most people resigned themselves to this fictitious truth,
accepting the chance they were given by the government not to have to know the
real cause of death. Later on, this same social phenomenon -- in which crimes
were committed in semi-obscurity and a certain amount of looking the other way
was required -- is what helped facilitate the Holocaust. The
murderers who began the euthanasia program in 1939 were surprised at how little
resistance they encountered. It had to do with the shame many family members
felt.
SPIEGEL: A sense of shame that still exists today.
Aly: One in eight Germans is directly related to someone who
became a victim of these murders. And if you include relatives by marriage,
this would apply to almost everyone. But it was not discussed in most families.
The murder victims have been forgotten.
SPIEGEL: Relatives can search the archives.
Aly: The institutions that maintain the files on the victims
today usually don't publicize the names, even though there are no privacy
concerns involved. I asked the president of the federal archive and the federal
data protection commissioner why. Both answered: "Please have
consideration for the relatives who are still alive." In the case of the
Jews, we would never suppress names. But with the so-called crazy people, we're
suddenly told that we want to protect their present-day relatives. Why? From
what?
SPIEGEL: It's the relatives' fear that perhaps they too have
something in them that isn't quite normal.
Aly: That's right. When the first memorials were created 20 years
ago and relatives began sending in their first letters, their main concern was:
Do we have a genetic disorder in the family?
SPIEGEL: In your book, you quote a father who, in the Nazi period,
expected the director of an institution to relieve him of responsibility for
his child. This extreme coldness seems disconcerting to us today.
 |
| Nazi euthanasia victims |
Aly: The extreme nature of it does, but the underlying feeling
of being burdened doesn't. My father had dementia for many years before he was
put in a nursing home. We knew it wasn't ideal, but there was no other option.
And here's another example: When a group of roommates and I parted ways 35
years ago, one of us ended up in a mental hospital. The rest of us still get
together today, but we don't talk about that person. We don't even know if he's
still alive. I mean, the mentally ill aren't exactly easy. When a child becomes
mentally ill, there can be a lot of finger-pointing in families.
SPIEGEL: Many disabled
fetuses are aborted. On the other hand, there is an effort to integrate the
disabled, and schools are being asked to participate in this effort. In that
sense, today's society differs considerably from the way it was in those days.
Aly: That's true. Karline and we, (her) parents, received a lot
of help from government agencies, and we were treated very kindly by private
individuals and professionals. It's often said that not enough is done, but
that's not true. All I can say is: Thank you. In this respect, we live in a
fortunate country. As the father of a disabled daughter, I know how important
that support is for inner balance. In the Nazi era, the relatives felt the
pressure of propaganda. They were seen as being very burdened themselves, most
suffered material hardships and, moreover, there was a war going on. I can
understand how people could falter under those circumstances.
SPIEGEL: Your
daughter, Karline, was born healthy and fell ill a few days thereafter. What
happened?
Aly: When she was
three days old, she got a streptococcus infection and wouldn't drink. Some 30
percent of pregnant women have streptococcus B, and if it's detected early on
and antibiotics are administered, everthing's fine. These tests weren't common
in the 1970s. Besides, it was the era of soft births. Karline was born in a
private clinic. They called the pediatrician on the phone, but he downplayed
the problem, calling it thirst fever. Karline's condition worsened by the hour.
She was thriving in the morning, but by the evening she looked gray, pale and
wrinkly. It took too long to transfer her to the children's hospital.
SPIEGEL: Was it the
doctor's mistake?
Aly: Yes, but, as
the parents, we were the ones who wanted the soft birth. Still, this sort of
thing will always happen, in one way or another. Disabilities are part of life;
it's just that their nature changes. A case like Karline's is rarer today, and
90 percent of unborn babies with Down syndrome are aborted, but premature
births cause more problems today, for example. And there are also more elderly
people with serious dementia.
SPIEGEL: How did the
doctors react in your case?
Aly: The head of
the ICU at the university hospital took me aside after three days and said:
"If your daughter survives the next night, she'll be severely
disabled." I understood it as a coded question, and I remember it as if it
were yesterday.
SPIEGEL: You mean as a
question as to whether the doctors should make sure that Karline didn't survive
the night? What did you say?
Aly: That he
should do everything possible to help her survive.
SPIEGEL: Even before
Karline's birth, the plan was that she would live with her mother. The mother,
Morlind Tumler, has a child from another relationship, and you have three
children from your marriage. How did Karline change your life?
Aly: I want to
stress that Karline's mother assumed the lion's share (of the work). She took
the first year off from work, but then she went back to her job as a teacher at
what was an inclusive school for the time. And, of course, Karline gave me the
impetus for my work.
SPIEGEL: You seem
happy when you talk about Karline, and yet life with a disabled child is
exhausting.
Aly: Karline is unable to speak. She's in a wheelchair, she has
no control over her movements, her upper body has to be supported and she
sometimes has epileptic seizures.
SPIEGEL: She has to be
fed, diapered and sometimes carried?
Aly: Yes, but
she's small and delicate. She only weighs 20 kilograms (44 lbs.), which is
advantageous. I don't believe that life with a severely disabled child is more
tedious than life with a child who isn't as limited. I even think that parents
can have far more trouble coping with a moderately disabled child. They try for
years and organize dozens of treatments before accepting their child for what
he or she is.
SPIEGEL: And, in
Karline's case, was it clear from the beginning that there would be little
improvement?
Aly: After about a
year. So it was easier for us to say: Okay, we'll try to make life as easy as
possible for the child. It isn't unusual for parents to develop aggression
toward a disabled child -- or even to wish death upon them. It's the result of
feeling overburdened, abandoned and desperate. Such ambivalent feelings are a
heavy burden on our conscience because they are directed against a person who
is close to us and is also completely vulnerable. The Nazis' emphasis on health
and fitness amplified this quite human ambivalence and set the stage for a
policy of murder.
SPIEGEL: Parents hope
to see themselves reflected in their children. It's one of the ways they
establish a bond. When a child is gifted, parents like to believe that it's
because of them. It must be more difficult to see yourself in a disabled child.
Aly: (This type of
bonding) definitely works. Karline is very gentle and even-tempered, which she
certainly gets from her mother. She's pretty. She laughs and cries, and she
loves music, good food and company. She also drinks a beer once in a while. She
looks mischievous at times, and then we say that she looks very intelligent.
SPIEGEL: Your daughter
went to an alternative kindergarten and then a special school, and today she
lives in a supervised group home. How do you feel about the most recent efforts
to achieve inclusion, meaning that all schools should be open to all children?
Critics say that when disabled children are sent to mainstream schools, they
are more likely to feel different from the norm and suffer even more as a
result.
Aly: There are
children who recognize that they have a special role, and they enjoy it. But
there are also many who sense that they can't do what the others can do, and
they're happy to be placed in a protected school. It depends on their
personalities. That's why it should be a matter of choice.
SPIEGEL: The call for inclusive schooling tends to come from the
left-leaning part of society. You too were once a protagonist of the leftist
movement, but you have now distanced yourself from some of its causes. You
write in your book that the ideology that leads to euthanasia was inspired by
the reform movement, which essentially came from the left. What brought you to
that realization?
 |
| White Rose campaign members |
Aly: There was no
resistance to the euthanasia murders from the leftist or secular side of
society. The notion of a healthy society, of capable people who are able to
enjoy life, arose in the liberal, middle-class, leftist and non-religious
segments of society. The euthanasia idea came from neither the radical
right-wing nor the conservative corner. It was and remains part of the modern
age and progressive thought. It's just that nowhere in the world was this way
of thinking put into practice quite as radically as in Nazi Germany. Assisted
suicide is a very accepted practice in some European societies that are closely
oriented toward modernity.
SPIEGEL: Which ones?
Aly: I recently
met with a Dutch colleague. She said that she had just been on the phone with
her siblings to schedule a date for the assisted suicide of their mother, who
has cancer. The son of the Dutch queen has been in a coma since he had a skiing
accident, and he is being cared for in England because there are almost no
facilities left in the Netherlands that handle such patients.
SPIEGEL: The
Netherlands was the world's first country to legalize active assisted suicide.
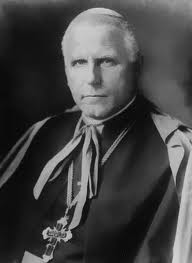 |
| Cardinal von Galen |
Aly: That's
consistent with the country's history. The Dutch were the first modern
bourgeois society in Europe. At an early date, they stressed
self-determination, worldly happiness and prosperity.
SPIEGEL: Resistance
against the destruction of so-called worthless life came from the church,
specifically Clemens August Graf von Galen, who was bishop of (the northern
German city of) Münster from 1933 to 1946. Galen was very conservative. This
shows that euthanasia can hardly be associated with categories like left and
right.
Aly: In the same
sermon in which he denounced euthanasia as a serious crime, Count Galen also
raged against premarital sex. The motives behind Galen's resistance are foreign
to us today, and yet his singular, courageous resistance is worthy of
admiration.
SPIEGEL: Most of us
want to live autonomous lives and tolerate abortion and assisted suicide under
certain circumstances. At the same time, we know that the model of perfection
turns us into monsters. The church is losing influence, leaving a void where
moral guidelines are concerned. Do we need new ethics?
Aly: Yes, we have
to reformulate moral standards. Human beings have to impose limits on
themselves when it comes to their actions and desires. There is a beautiful and
very radical notion in the bible: Man is made in the image of God, no matter
how sick, poor or damaged he is. We should try to transpose this maxim to our
secular and constitutional self-image.
SPIEGEL: Mr. Aly,
thank you for this interview.
Interview conducted by Susanne
Beyer, translated from the German by Christopher Sultan


 Suicide was decriminalised in Ireland in 1993, but Section 2.2 of the Criminal Law Suicide Act 1993 makes it an offence to ‘aid, abet, counsel or procure’ a suicide. Those convicted under this law still face a custodial sentence of up to 14 years.
Suicide was decriminalised in Ireland in 1993, but Section 2.2 of the Criminal Law Suicide Act 1993 makes it an offence to ‘aid, abet, counsel or procure’ a suicide. Those convicted under this law still face a custodial sentence of up to 14 years.


















